We offer courses in Canada and the US. If you are experiencing issues with our website and need help to register, or if you have questions, please call us at 866-291-9121.
If you are facing any issues with your online course, registration, or training, please click here to submit a help request.
If you are facing any issues with your online course, registration, or training, please click here to submit a help request.
CPR Week 2026, officially National CPR and AED Awareness Week, runs June 1 to 7. For a teen or adult who suddenly collapses, skip the pulse check: confirm the person is unresponsive and not breathing normally, call 911, and push hard and fast in the center of the chest at 100 to 120 compressions per minute. Hands-only CPR is recommended for untrained bystanders helping a collapsed adult, while rescue breaths still matter for infants, children, and drowning or overdose emergencies.
CPR Week 2026
7 in 10 Cardiac Arrests Happen at Home
The person whose life you save is most likely someone you love. Get certified this CPR Week.
out-of-hospital cardiac arrests in the US each year
7 in 10
happen at home, not in public or at a hospital
2x to 3x
higher survival when a bystander starts CPR immediately
Picture CPR and you probably imagine a 1990s TV scene: two fingers on the neck, a panicked “There’s no pulse,” then dramatic rescue breaths. That script is outdated, and in a real emergency it could cost a life. CPR Week 2026 is as much about unlearning as learning. Here are the five rules that have changed, and what each one means in practice.
Quick Reference: What Changed
Here are the five biggest updates. The rest of this article explains each one.
What you may have learned
The 2026 reality
Check for a pulse before you start.
Skip the pulse. Look for breathing; if unresponsive, start compressions.
Mouth-to-mouth is required.
Hands-only CPR for untrained bystanders helping a collapsed adult.
CPR is different for women.
The technique is identical. Hands go in the center of the chest.
Stop if you hear a crack.
Keep pushing. Rib injuries happen but they heal.
An AED could shock the wrong person.
AEDs analyze the rhythm first. They will not shock a healthy heart.
What Is National CPR Week, and When Is It in 2026?
CPR Week 2026, formally National CPR and AED Awareness Week, runs June 1–7 under a 2007 Congressional resolution. The American Heart Association leads the national effort with free classes and community campaigns, and many accredited training providers run certification and recertification classes throughout the week. Whether you call it CPR Week, CPR Awareness Week, or cpr aed awareness week, the goal is the same: replace the outdated version in your head with the current science. More than 1,600 people experience cardiac arrest each day in the U.S. Bystander CPR can double or even triple survival rates — which is exactly why this week exists.
Why Does Outdated CPR Knowledge Put Lives at Risk?
About 350,000 Americans have an out-of-hospital cardiac arrest each year, and roughly 90 percent do not survive. Every minute a cardiac arrest victim goes without intervention, survival odds plunge by 7% to 10%, but immediate bystander CPR slows that drop to 3% to 4% per minute. The barrier is mainly the outdated, complicated script most people carry in their heads, even though the importance of immediate action during a cardiac emergency is the ultimate factor in survival. The October 2025 AHA Guidelines keep stripping that complexity away. A classroom CPR and AED course is the fastest way to build real confidence. Roughly 70% of sudden cardiac arrests happen at home or in private residential settings. When a person’s heart stops beating, their chance of survival drops by roughly 10% for every minute without intervention. Certified courses teach the proper use of chest compressions and an AED together, which can significantly increase survival rates.
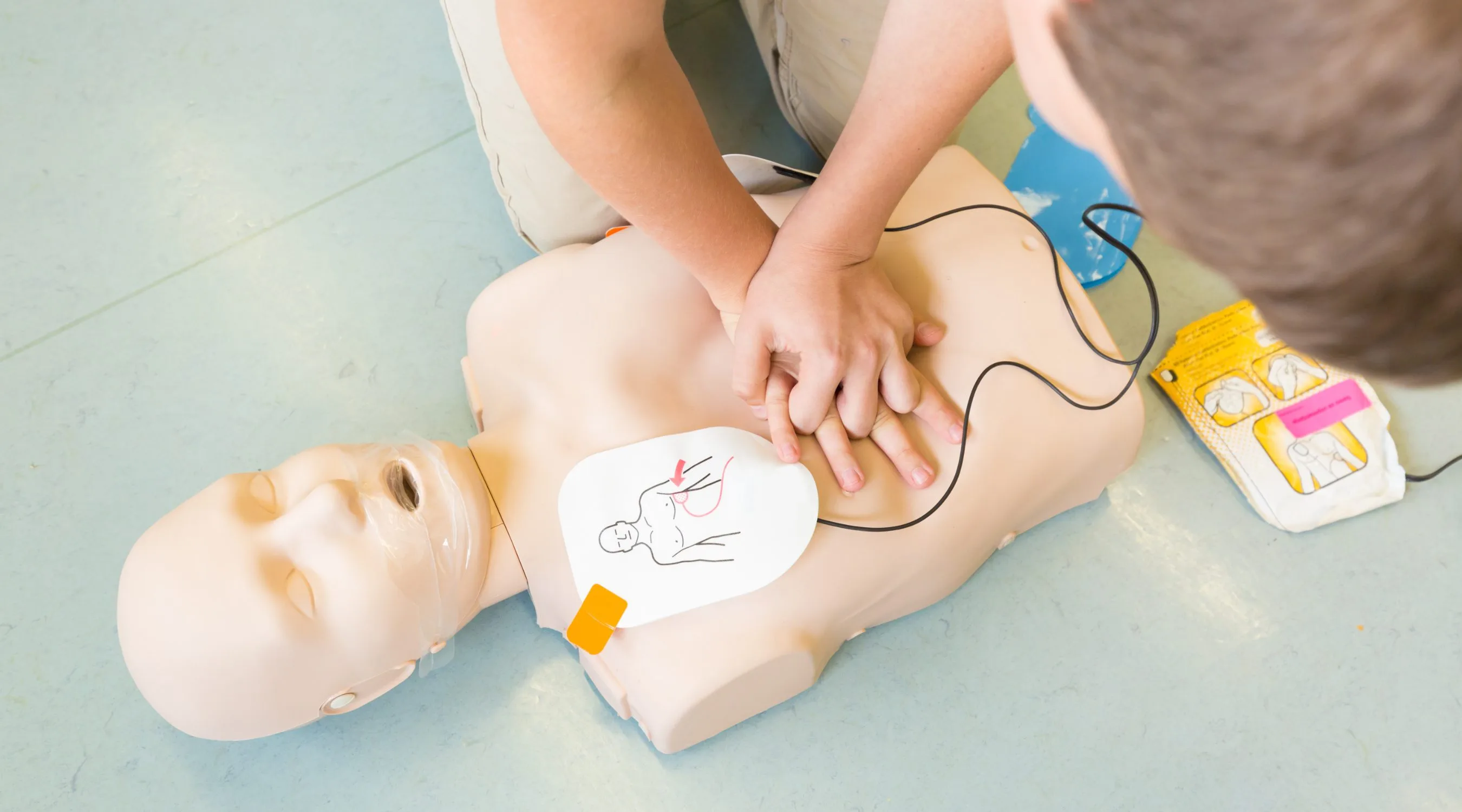
Hands-On Practice
Reading the Steps Is Not the Same as Doing Them
Practice the 2026 technique on a manikin with a certified instructor near you.
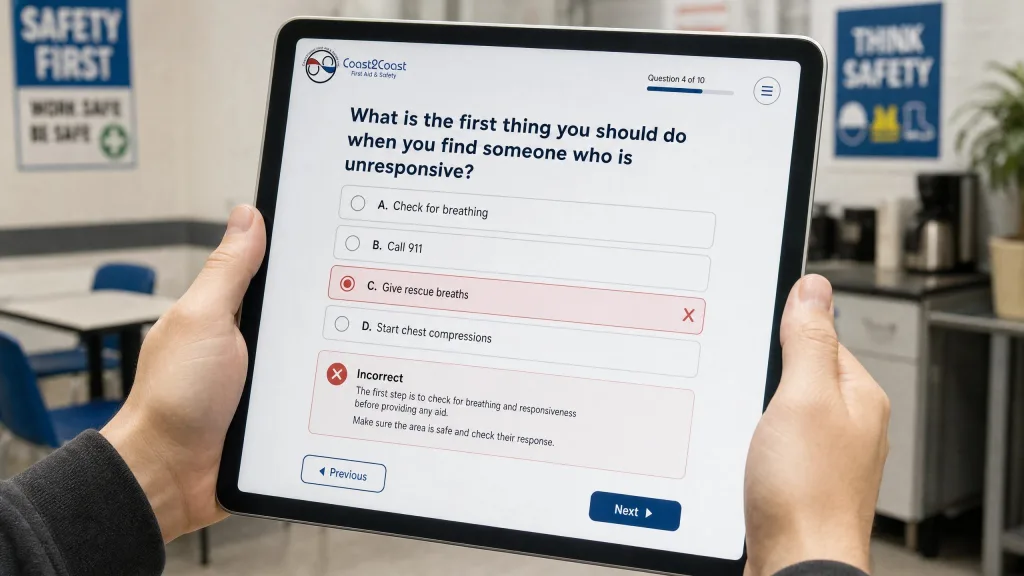
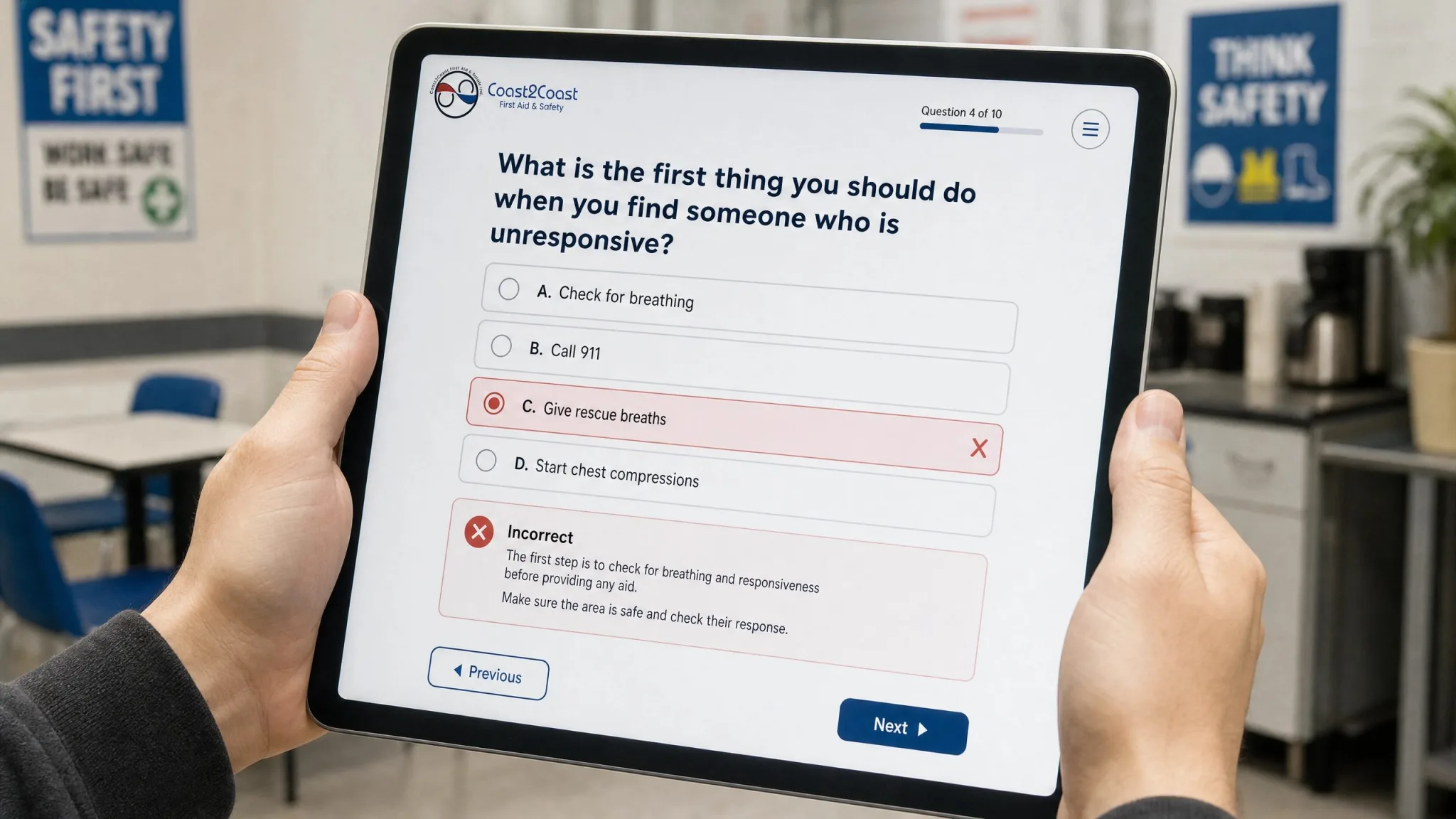
For decades, training told you to find a pulse before compressions. The 2026 reality: skip it. Under adrenaline, your own pulse is easy to feel in your fingertips and easy to mistake for the victim’s, and checking burns seconds. Tap the shoulder and shout, look at the chest for 5 to 10 seconds for normal breathing (gasping does not count), and if the person is unresponsive and not breathing normally, call 911 and push hard and fast in the center of the chest. If you are alone, put 911 on speaker first.
Safety Tip: Set your compression tempo to 100 to 120 beats per minute, roughly the rhythm of “Stayin’ Alive.” Push at least two inches deep and let the chest fully recoil between compressions so the heart can refill.
Do You Still Need to Give Rescue Breaths?
For many bystanders, mouth-to-mouth is the biggest barrier to acting. Many bystanders also hesitate because they lack confidence or fear causing harm, which makes simple guidance especially important. The 2026 reality: for a collapsed teen or adult, hands-only CPR is recommended. At the moment of cardiac arrest the blood still holds an oxygen reserve, so the immediate problem is circulation, not oxygen. Every pause for breaths drops the pressure you built toward zero. Continuous compressions at 100 to 120 per minute, roughly the tempo of “Stayin’ Alive,” keep that blood moving to the brain, because brain damage can begin after just 4 minutes and death can occur within 4 to 6 minutes.
When Rescue Breaths Are Still Essential
Rescue breaths remain critical for infants, children, and victims of drowning or drug overdose, because those arrests typically start as a breathing problem, and sudden cardiac arrest can still arise in youth emergencies where rapid CPR and AED use matters. The 2025 AHA Guidelines reinforce this and note that children aged 12 and older can reasonably be taught CPR and AED use. It is also the number one cause of death in youth athletes. Safe Kids has partnered with Tina Charles on sports safety clinics that have reached over 1,000 child participants, underscoring why AED and CPR education matters in youth sports. If you care for children as a caregiver or parent or work near water, a full first aid and CPR course covering both compressions and rescue breaths is worth the time.
Should Women Receive CPR from a Bystander?
Research shows women who suffer cardiac arrest in public are significantly less likely to receive bystander CPR than men, due to fear of inappropriate touching and a false belief that female anatomy makes CPR harder. Both are myths. Cardiovascular disease is the leading cause of death in women, and the technique is identical for everyone. Place the heel of your hand in the center of the chest and push hard and fast. A woman’s breasts do not change hand placement. If using an AED, move clothing aside so pads sit on bare skin.
Put These Updated Rules Into Practice
Knowing CPR is step one, and practical instruction helps you feel prepared to act. A certified instructor puts those skills in your hands with real practice on a manikin, including AED training, so you can act without hesitation when it counts.
Learn This Skill in a Real Classroom
Hands-on manikin and AED practice with a certified instructor.
Fear of causing harm is one of the most common reasons many people hesitate to get involved and freeze. The 2026 reality: any CPR is far better than none. Effective compressions push at least two inches deep, and that force can crack a rib. But a person in cardiac arrest is clinically dead, so once you are involved, you cannot make it worse. A broken rib heals. Brain death does not reverse. If you feel a pop or hear a crack, keep going.
Are You Protected by Good Samaritan Laws?
Yes. All 50 states have Good Samaritan laws protecting bystanders who give emergency help in good faith, as long as they act reasonably and do not expect payment. You do not need certification to be covered. These laws exist so that fear of a lawsuit never stops someone from stepping in.
Can You Accidentally Shock Someone With an AED?
CPR keeps blood moving; an AED shocks a chaotic rhythm back toward normal. Many people fear opening the cabinet, worried they might shock someone who merely fainted. Modern AEDs prevent that: once on, a calm voice guides each step and the device analyzes the heart’s rhythm before allowing a shock. It only fires when one is needed, so you cannot shock a healthy heart. The bigger problem is access: only half of US workers can locate the nearest AED. Tina Charles, a WNBA All-Star, has also pushed for better AED access as part of community health preparedness to help prevent sudden cardiac arrest in youth athletes. Our team can help through the contact page.
How Can You Take Part in CPR Week 2026 (June 1–7)?
Until the ambulance arrives, you are the first responder, and the best use of CPR Week 2026 is to turn what you just read into a skill you can actually perform. Reading about chest compressions is not the same as feeling the right depth and rhythm under your own hands. The fastest way to close that gap is a short, hands-on class with a certified instructor, where you practice compressions and AED use on a manikin until they feel automatic. About 7 in 10 cardiac arrests happen at home, so the person you are training to help is most likely someone you love. Spend a few hours with us this week and walk out ready to act without hesitation.
CPR Week 2026
Come Take a Class With Us This CPR Week
A few hours with a certified instructor is all it takes to be ready when it counts. Reserve your seat today.
For CPR Week 2026: skip the pulse check, skip rescue breaths on a collapsed adult, give the same care regardless of gender, and use an AED without fear. Call 911, push hard and fast at 100 to 120 per minute, and deploy the AED as soon as one is available. It will not shock a heart that does not need it. Good Samaritan laws protect you in all 50 states.
Only Half of US Workers Can Find Their AED
Group CPR and first aid training closes that gap. Bring a certified instructor to your workplace this CPR Week.
A: CPR Week 2026 runs June 1 to 7. Formally called National CPR and AED Awareness Week, and sometimes listed as cpr aed awareness week, it falls on the first seven days of June every year under a 2007 Congressional resolution and is led by the American Heart Association. Its purpose is to encourage more people to learn CPR and AED use, raise awareness through public campaigns, and help more people save a life while updating the public on guidelines that have changed since they last took a class.
Q2: Why shouldn’t you check for a pulse before starting CPR?
A: Checking for a pulse wastes time and is unreliable for untrained responders. Under stress, your own heartbeat is easy to feel in your fingertips, which can fool you into thinking a victim’s heart is beating when it has stopped. Skip the pulse check entirely. Tap the person and shout, then look for normal breathing for 5 to 10 seconds. If the person is unresponsive and not breathing normally, call 911 and begin chest compressions right away.
Q3: What is hands-only CPR?
A: Hands-only CPR is cardiopulmonary resuscitation without mouth-to-mouth breaths. For a teen or adult who suddenly collapses, an untrained bystander pushes hard and fast in the center of the chest at 100 to 120 compressions per minute without stopping for breaths. It works because the blood still carries an oxygen reserve at the moment of collapse, so the priority is circulation. Removing the breaths also makes bystanders far more willing to act, and that can save a life.
More FAQs: Women and the Law
Q4: Is CPR different for women?
A: No. The technique is identical for women and men. Place the heel of your hand in the center of the chest, on the breastbone, and push hard and fast regardless of anatomy. A woman’s breasts do not change hand placement or interfere with compressions. If you use an AED, move clothing and undergarments aside so the pads sit on bare skin. Research shows women receive bystander CPR less often than men due to fear of inappropriate contact, and that hesitation costs lives.
Q5: Can you be sued for performing CPR without certification?
A: No. You do not need certification or medical credentials to legally perform CPR in an emergency. All 50 states have Good Samaritan laws that protect people who voluntarily give emergency aid in good faith, provided they act reasonably and do not expect payment. These laws exist specifically so that fear of liability does not stop bystanders from helping. The far greater risk is doing nothing, since a cardiac arrest victim who receives no CPR has very little chance of survival.
Disclaimer: This article is for general informational purposes only and does not replace professional medical advice or hands-on CPR and first aid training. Always call 911 in an emergency. For certification, take an accredited course with a qualified instructor.
About This Article and Our Sources
Written and reviewed by Ashkon Pourheidary, B.Sc. (Hons) Neuroscience and a certified first aid and CPR instructor since 2011. Reviewed against the 2025 American Heart Association Guidelines for CPR and Emergency Cardiovascular Care (Circulation, October 2025), the AHA 2025 Heart Disease and Stroke Statistics Update, and AHA CPR Facts and Statistics.
COAST2COAST FIRST AID · RESEARCH & INSIGHTS · MAY 2026
The Workplace Injury Costing California $2.2 Billion a Year Is Not the One Anyone Is Training For — New Data From 20,000+ Canadian Exams Shows Where Certified Responders Actually Fail
The workplace injury costing California an estimated $2.2 billion a year is not the one anyone is training for. Data from more than 20,000 written first aid exams from our Canadian certification network shows where certified responders actually fail — and why California, with no written knowledge assessment requirement, has no way to see it.
By Ashkon Pour-Heidary, HBSc Neuroscience · American Red Cross & Canadian Red Cross Instructor Trainer · Founder, Coast2Coast First Aid
May 2026 · c2cfirstaidaquatics.com/us/first-aid-knowledge-gap-report
This is the full analysis behind the press release issued May 2026. Want the shorter version? The press release lives at c2cfirstaidaquatics.com/press-releases
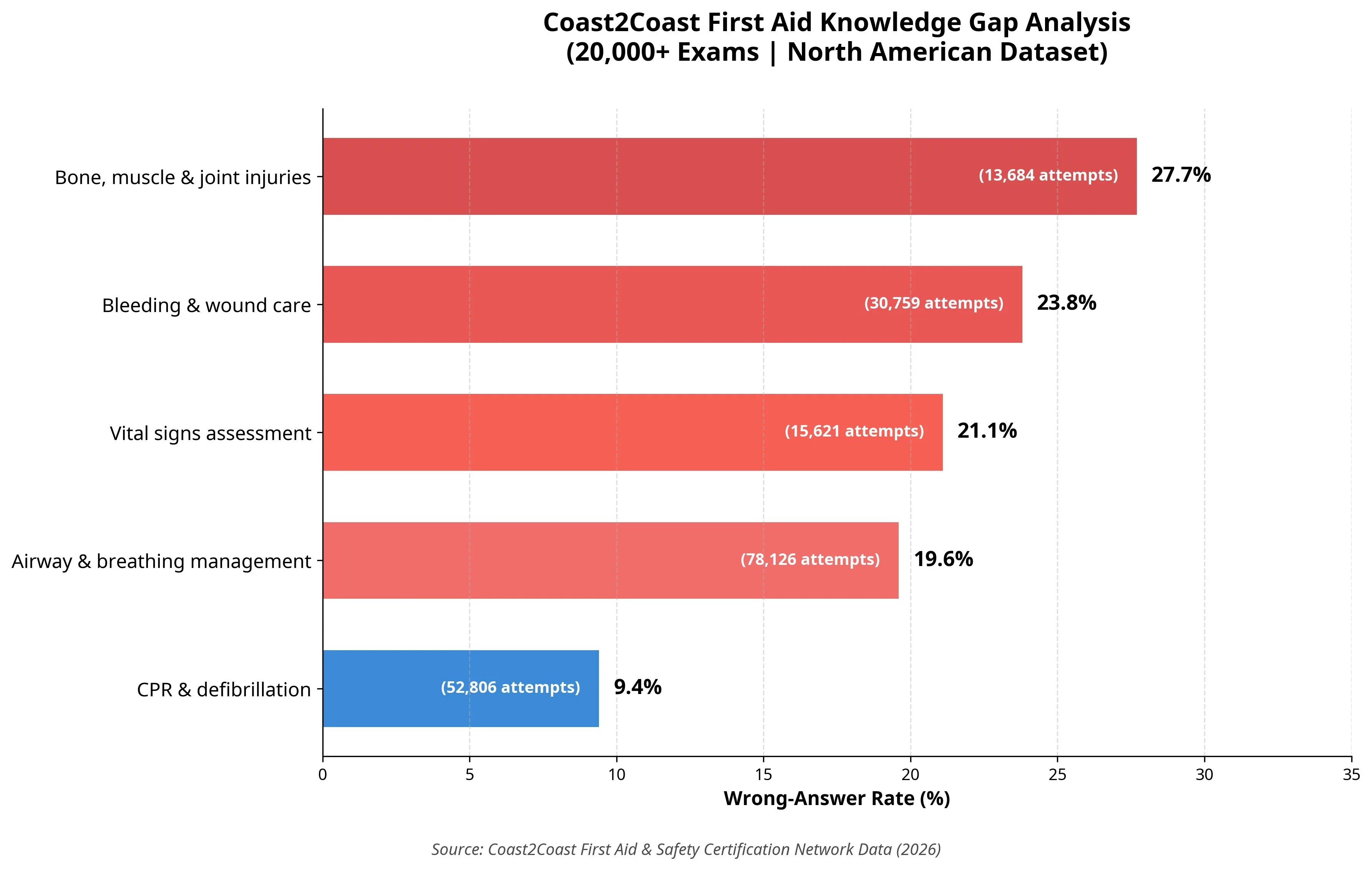
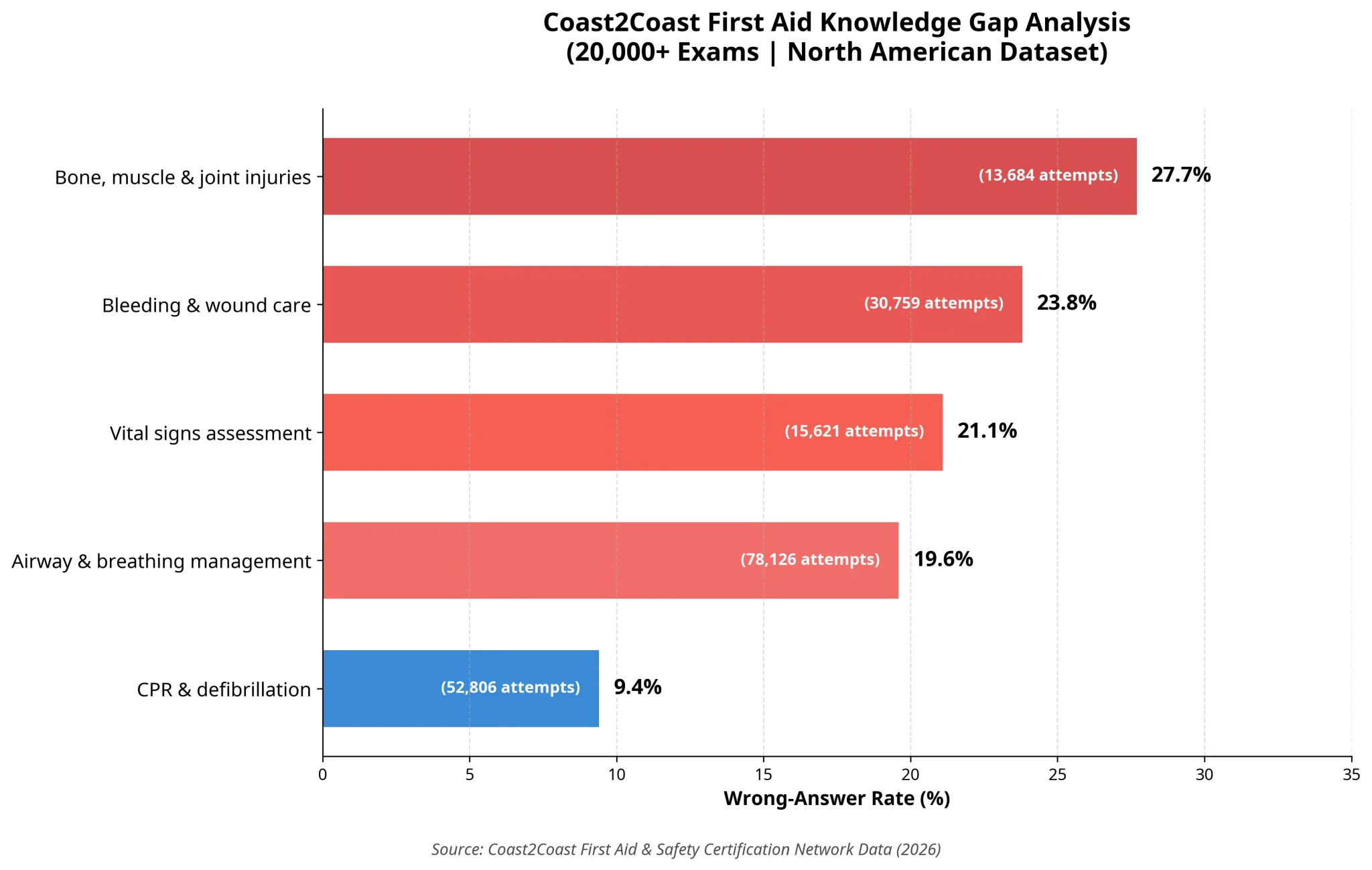
An analysis of more than 20,000 written first aid certification exams from Coast2Coast First Aid’s Canadian network shows that certified lay rescuers most often answer incorrectly on bone, muscle and joint injuries (27.7% wrong) and bleeding and wound care (23.8% wrong), far more often than on CPR and defibrillation (9.4% wrong). Because California does not require a written knowledge assessment for workplace first aid certification, it has no way to detect these same gaps. Coast2Coast is asking Cal/OSHA to add a written knowledge assessment to the Section 3400 standard, in addition to the existing practical skills demonstration.
27.7%
wrong-answer rate on bone, muscle & joint injuries
23.8%
wrong-answer rate on bleeding & wound care
9.4%
wrong-answer rate on CPR & defibrillation
There is a moment every first aid instructor knows. The student in front of you has just passed. They have the certificate. They are heading for the door. And somewhere in the back of your mind is a question you cannot fully answer: are they actually ready?
I know that question personally. I passed my first first aid course at 19. I had the card. When the moment came to demonstrate what I actually knew — a practical assessment for an emergency response team at the University of Toronto — I could not perform. The certificate said I was ready. I was not.
That experience is the reason Coast2Coast First Aid exists, and it is the reason we built the technology to finally answer that question at scale.
Why We Built This Platform — First, For Ourselves
We need to be clear about something up front: we did not build this digital testing platform to publish research. We built it because we run a training organization that cares whether its students actually learn what they came to learn — and we needed answers we could not get from paper exams that end up filed in a drawer.
Coast2Coast First Aid co-founder Aryan Sekhavati built the proprietary in-classroom testing platform — the first of its kind among first aid and CPR training providers in North America — to capture written exam responses in real time across every classroom in the network. Before this platform existed, exam responses were graded on paper, filed away, and never aggregated. We use the data it generates in three ways, every day, internally:
First, we look at network-wide question patterns. Which specific questions produce the highest rate of wrong answers across thousands of students? That tells us where our curriculum needs more time, more scenarios, more reinforcement. It is a signal we cannot get any other way.
Second, we look at classroom-level concentration. Is the gap broad across the network, or concentrated in specific classrooms? Broad patterns drive curriculum revision. Concentrated patterns drive targeted support to specific locations.
Third, we look at instructor baseline data. Every instructor has a network-wide expected range based on student outcomes. When a specific instructor’s student results consistently fall outside that range, the data prompts a coaching conversation — lesson plan review, time on high-miss topics, an improvement plan. Not a disciplinary process. A development one, driven by what the data shows.
This is internal quality assurance. It is how we make sure our students get what they came for, and how we make sure our instructors are set up to succeed.
But the more data we accumulated, the clearer one thing became: the knowledge gaps we were finding were not random. They were patterns. Consistent. Stable across thousands of students. Pointing at the same topics, again and again. That is when we decided to share what we were seeing publicly — because the implications go beyond our own classrooms.
We will soon make a version of this platform available to our California students. Those enrolled in first aid and CPR courses in Los Angeles will have the option to complete an in-class knowledge quiz to solidify their understanding and be better prepared for real-world emergencies — giving California workers the same feedback loop that has been driving improvement in our Canadian network. Our intent is to publish California-specific data as it accumulates, with the same transparency as this report.
What 20,000 Exams Show
The industry’s attention has long centered on CPR. Chest compressions, AED use, airway management — these dominate public awareness, instructor training time, and regulatory conversation. The data from more than 20,000 digitally captured certification exams in our network confirms that focus is working. Questions related to CPR and defibrillation produce an incorrect answer rate of just 9.4%.
The topics producing consistent wrong answers — in patterns stable enough across thousands of students to act on — are the ones nobody is talking about.
About this data. These exam responses were captured between July 2025 and May 2026 across our Canadian certification network. The primary dataset covers the Standard First Aid & CPR/AED Level C cohort [13] — the Canadian equivalent of the American Red Cross Adult and Pediatric First Aid/CPR/AED course [12] that California employers accept for workplace compliance under Cal/OSHA Title 8, Section 3400. [11] That regulation is where this entire policy conversation begins, and where we will return at the end.
Two Knowledge Gaps That Matter Most in the Workplace
We want to focus on two findings specifically, because they are where the data most directly intersects with the kinds of injuries that happen on California worksites every day.
Bone, muscle and joint injuries — 27.7% wrong-answer rate
Among the 13,684 attempts we analyzed in this category, more than one in four lay rescuers — the term used in workplace safety regulations for a non-healthcare employee trained in first aid — answered the bone and muscle injury question incorrectly. These were students who attended the course, sat the exam, and passed certification.
Incorrect bone and muscle response is not a neutral outcome. Moving a patient before stabilizing a fracture can turn a contained break into a displaced or compound injury, escalating it from a splint-and-monitor situation into a surgical one. Failing to recognize when not to move someone risks secondary injury, including potential spinal complications. Incorrect immobilization can extend recovery time and increase the risk of long-term impairment.
This matters in California specifically because musculoskeletal disorders are the leading category of workplace injuries in the United States, with 937,620 DART cases reported in 2023–2024. [3] California tracks its own state-specific injury data through the California Survey of Occupational Injuries and Illnesses, administered by the California Department of Industrial Relations in cooperation with the U.S. Bureau of Labor Statistics — the same SOII methodology that produces the national figures. [14] Given that the same injury categories dominate workplace injuries nationally, it is reasonable to expect they do in California as well.
Bleeding and wound care — 23.8% wrong-answer rate
Across 30,759 attempts — by far our largest dataset for any single category — nearly one in four lay rescuers gave the wrong answer to questions about bleeding and wound care. This is significant because hemorrhage control is consistently identified in peer-reviewed research as one of the most critical and most poorly performed lay-rescuer interventions.
A systematic literature review published in Acta Anaesthesiologica Scandinavica found that incorrect first aid was administered in up to 83.7% of cases by lay rescuers to trauma victims, with airway handling and hemorrhage control specifically identified as particular areas of concern. [2] The same review estimated that correct first aid could have reduced mortality by 1.8–4.5%.
Incorrect wound care has direct consequences in workplace settings: a wound that could have been controlled at the first aid level escalates into one requiring medical treatment beyond first aid — turning a non-recordable incident into an OSHA recordable claim. Inadequate hemorrhage control in serious cases is life-threatening. The training is supposed to address these scenarios. The data suggests that, even with certification, almost a quarter of trained lay rescuers cannot reliably answer the underlying knowledge question.
What these two findings have in common: they are both about the kinds of routine, common workplace injuries that ordinary lay rescuers will actually encounter. They are not exotic scenarios. They are the everyday situations the training is supposed to prepare them for. And the data shows that, across thousands of students, the training is not consistently doing that — not at a level our network can see, and certainly not at a level California has any way to measure.
Why We Believe California Has the Same Gaps
We need to be transparent: the 27.7% and 23.8% figures come from our Canadian network. We cannot tell you California’s exact rate, because California does not require a written knowledge assessment for lay rescuers. There is no California number to publish. What we can show, however, is that the conditions producing these gaps are present in California for five independently verifiable reasons.
The curriculum is similar.
American Red Cross and Canadian Red Cross first aid courses are both built on the guidelines of the International Liaison Committee on Resuscitation — the same international evidence body, the same review cycle, the same underlying science. [10] The correct answer to “what do you do when a wound dressing saturates with blood” is the same in Los Angeles as it is in Toronto.
The certification framework is comparable.
The American Red Cross Adult and Pediatric First Aid/CPR/AED course — what California employers accept for workplace compliance [12] — is the US equivalent of the Canadian Standard First Aid & CPR/AED Level C course in our dataset. [13] Both operate under the same international Red Cross movement, the same certification methodology, the same ILCOR standards. The main difference is that in Canada this course takes about 14–16 hours, while in the United States the course averages 4–6 hours depending on class size. That difference matters: if the same knowledge has to be transferred in roughly a third of the time, the gaps our written assessment reveals are likely to be at least as severe in the United States — possibly more so.
Human physiology does not change at the border.
The cognitive decisions our data shows lay rescuers struggle with — when to stabilize before moving, when to apply a sling, what to do when a wound dressing saturates, when to call for additional help — are difficult under pressure for the same reasons in any jurisdiction. The difficulty is not cultural. It is a function of how the material was taught, how much scenario practice the student got, and whether anyone measured what they retained. None of those variables are specific to Canada.
The workplace injury patterns are the same.
Musculoskeletal disorders are the leading category of US workplace injuries — 937,620 DART cases reported by the Bureau of Labor Statistics in 2023–2024. [3] California participates in the same Survey of Occupational Injuries and Illnesses methodology, with state-specific data published by the California Department of Industrial Relations. [14] Bleeding and wound care issues are routine workplace events across construction, manufacturing, hospitality, healthcare support, and warehousing. The categories where our data shows the biggest knowledge gaps are exactly the kinds of injuries California workplaces report regularly.
We are in California now, teaching the same program.
Coast2Coast First Aid has operated in Los Angeles since November 2025. We use the same curriculum, the same testing methodology, and the same instructor standards in our California classrooms that produced this dataset. We do not yet have enough US exams to publish California-specific numbers, but our intent is to. When we do, we will share that data too — with the same transparency. However, as apposed to the Canada where our students are required to complete the test, in California, we are unable to make this mandatory, making a head wind for data collection.
What’s at Stake Financially
The relationship between first-aid knowledge and injury outcomes is not a clean dollars-in, dollars-out equation — real workplace injuries are caused by many factors, and no single training improvement produces a guaranteed financial return. What the research does consistently show is the same shape: better-prepared lay rescuers correlate with better outcomes for injured workers, and better outcomes translate into measurable financial benefit across the system.
937,620
Musculoskeletal disorder DART cases in US, 2023–2024 [3]
$20B+
Direct workers’ comp costs for MSDs annually (OSHA/NIOSH)
~$2.2B
California’s estimated share (approx. 11% of US workforce)
69M
US workdays lost to injury in 2024 (NSC) [6]
How better-prepared lay rescuers shift outcomes.
OSHA’s 2012 white paper on Injury and Illness Prevention Programs documents that workplaces implementing comprehensive prevention programs — which include emergency response and first aid capability as core elements — typically see workplace injury and illness rates reduced by 15 to 35 percent. [1] Verified first aid knowledge is one piece of that larger picture, but it is a piece California currently has no way to measure.
When a lay rescuer responds effectively to a workplace injury, the injury tends to stay manageable. The worker recovers faster. The claim stays smaller. The team returns to baseline sooner. When a lay rescuer does not have the knowledge — when they move a patient who shouldn’t be moved, miss the signs of a serious injury, or apply incorrect wound care — the same injury can escalate, with direct workers’ compensation consequences. The average workers’ compensation claim for all injuries is $47,316. For fracture, crush, or dislocation injuries, it averages $66,467. [7]
OSHA’s official Safety Pays calculator documents that indirect costs of a workplace injury — overtime to backfill the role, hiring and training a temporary replacement, supervisor and HR time, OSHA documentation, team disruption — range from 1.1 times the direct cost for severe injuries to 4.5 times the direct cost for less severe ones. [5] Other OSHA materials describe these indirect cost categories in detail. [6] Median time away from work for a serious musculoskeletal injury is 8 days, and California employers carry claims history through the experience modification factor (X-mod), which influences premium pricing over a multi-year period. California’s benchmark advisory premium rate is currently $1.38 per $100 of payroll. [8]
Lets be clear, we are not asserting that any single training improvement produces a fixed dollar return. We are saying that the research consistently shows the same shape: when lay rescuers are better prepared, injuries stay contained more often, recoveries are faster, and financial pressure on the system eases. OSHA and ASSP research on well-implemented safety programs has cited returns ranging from $4 to $6 per dollar invested. [9] Verified first aid knowledge — measured, tracked, and improved over time — is part of that picture.
What This Means — and What We’re Asking California to Consider
Let us return to the question we opened with — the one every first aid instructor knows, the one I could not answer as a student myself: are they actually ready?
We built this platform to answer that question for our own organization — to know which curriculum topics need more time, which classrooms need targeted support, which instructors would benefit from coaching. That work is internal, ongoing, and is the reason we believe our network is in a position to share findings like these credibly.
But the same data has shown us something we cannot ignore. California — the state where we now operate and where we are committed to growing — has no equivalent way to see this layer of the certification picture. No one does. And that is a problem worth fixing.
Cal/OSHA Title 8, Section 3400 currently requires that workplace lay rescuers be “adequately trained to render first aid” at a standard equal to the American Red Cross. [11] Adequacy is measured through demonstrated physical skills — compressions, wound dressing, patient positioning. Those tests are essential and must not be replaced. They tell you whether someone can perform the technique.
What physical demonstration cannot reach is the cognitive layer underneath. When to act. In what order. What to do when the first approach doesn’t work. Whether the lay rescuer recognizes the signs of a serious bone or muscle injury, knows what to do when a wound dressing saturates with blood, and understands why the order of operations matters. Those are knowledge questions. They can only be measured by asking them.
Without that measurement, California has no way to know whether its certified lay rescuer workforce is actually prepared for the cognitive demands of a workplace emergency — only that they were able to demonstrate physical skills in a controlled setting. Skill demonstration and knowledge assessment are not redundant. They are complementary. Together they answer two different questions: “can this person perform the procedure?” and “does this person understand when, why, and how to apply it?” Both need answering.
Our specific request: We are asking Cal/OSHA and the California Occupational Safety and Health Standards Board to consider adding a written knowledge assessment requirement to the standard for workplace first aid certification under Section 3400 — in addition to the existing practical skills demonstration, not in place of it.
Why this matters for California: Coupling a written knowledge assessment with the physical skills test would close a measurement gap that currently makes it impossible for California to know whether certified lay rescuers are genuinely ready. It would create a feedback loop that drives continuous improvement in workplace safety training across the state — the same loop our internal platform creates for our organization. And it would put California at the front of a national standard worth leading on.
This is not a regulatory burden. The infrastructure exists. The methodology is proven. The American Red Cross already builds written knowledge content into its curriculum. What is missing is the requirement that it be measured.
We are sharing this data because we believe California is the state that takes this step first. The technology is in place. The argument is on the page. The decision is one regulatory action away.
“We built this platform to support our students, our instructors, and our internal quality. What it has shown us has implications well beyond our own classrooms. Our Canadian network data, drawn from more than 20,000 exams where written assessment is already standard, shows the gap is real and concentrated exactly where it hurts most. If knowledge gaps exist at these rates in a program with rigorous written testing, they are unlikely to be smaller in California, where no written test exists at all. California has the opportunity to set a standard that ensures every certified lay rescuer in the state — every person trained to help a coworker when something goes wrong — has demonstrated not only that they can perform the skill, but that they understand when and how to apply it. That is what genuine readiness looks like. And that is what California’s workers deserve.”
— Ashkon Pour-Heidary, HBSc Neuroscience · American Red Cross & Canadian Red Cross Instructor Trainer · Emergency Medical Responder Instructor Trainer · Founder, Coast2Coast First Aid
Key Takeaway
The most dangerous workplace first aid knowledge gaps are not in CPR. They are in the routine injuries lay rescuers actually encounter most: broken bones, sprains, and bleeding. California cannot currently measure these gaps because it requires no written knowledge assessment. Adding one to the Cal/OSHA Section 3400 standard, alongside the existing skills demonstration, would close that blind spot.
Workplace Training
Train Your Team With Verified, Measured Knowledge
Coast2Coast delivers first aid and CPR training to California workplaces using the same curriculum and standards behind this report.
Every claim in this report is linked to its source below. Reference numbers in the text are clickable. Each entry includes a direct URL to the original.
Tannvik TD, Bakke HK, Wisborg T. “A systematic literature review on first aid provided by laypeople to trauma victims.” Acta Anaesthesiologica Scandinavica, 2012. Incorrect first aid was given in up to 83.7% of cases; airway handling and haemorrhage control were particular areas of concern; correct first aid could have reduced mortality by 1.8–4.5%. https://pmc.ncbi.nlm.nih.gov/articles/PMC3495299/
OSHA Safety Pays Individual Injury Estimator — Background. Indirect-to-direct cost ratio ranges from 4.5× for minor injuries (direct costs under $3,000) to 1.1× for more severe injuries (direct costs over $10,000). Indirect costs include lost productivity, training replacement workers, overtime, accident investigation, and administrative burden. https://www.osha.gov/safetypays/background
OSHA. “Business Case for Safety and Health — Costs.” Indirect costs include training replacement employees, investigation, lost productivity, administrative burden. https://www.osha.gov/businesscase/costs
National Council on Compensation Insurance (NCCI), reported via NSC Injury Facts. Average cost for all workers’ comp claims, 2022–2023: $47,316. Fracture/crush/dislocation category average: $66,467. https://injuryfacts.nsc.org/work/costs/workers-compensation-costs/
International Liaison Committee on Resuscitation. American Red Cross and Canadian Red Cross first aid curricula are both built on ILCOR evidence guidelines. https://www.ilcor.org
California Code of Regulations, Title 8, Section 3400. “Medical Services and First Aid.” Employees must be adequately trained to render first aid, with training equal to that of the American Red Cross. No written knowledge assessment is required. https://www.dir.ca.gov/title8/3400.html
American Red Cross. “Adult and Pediatric First Aid/CPR/AED” course. The OSHA-compliant workplace first aid course in the United States. Typical duration: approximately 4–6 hours including online portion and in-person skills session. https://www.redcross.org/take-a-class/classes/adult-and-pediatric-first-aid%2Fcpr%2Faed/LP-00005000.html
Canadian Red Cross. “Standard First Aid & CPR/AED Level C” course. The Canadian equivalent of the US Adult and Pediatric First Aid/CPR/AED course. Typical duration: 14–16 hours of in-person instruction. https://www.redcross.ca/training-and-certification/course-descriptions/first-aid-training/standard-first-aid-cpr
California Department of Industrial Relations, Office of Policy, Research and Legislation. Nonfatal Occupational Injuries and Illnesses in California — Survey of Occupational Injuries and Illnesses (SOII), administered jointly with the U.S. Bureau of Labor Statistics. State-specific data on workplace injury counts and incidence rates by industry, case type, and worker characteristics. https://www.dir.ca.gov/oprl/nonfatal.htm
About Coast2Coast First Aid
An authorized American Red Cross Training Partner and an American Heart Association Aligned Training Site operating across North America, with Los Angeles operations established in November 2025. Founded in 2014, the company has certified more than 150,000 individuals. Founder Ashkon Pour-Heidary holds a Bachelor of Science in Neuroscience (University of Toronto) and is a certified Instructor Trainer for both the American Red Cross and the Canadian Red Cross, as well as an Emergency Medical Responder Instructor Trainer.
Full dataset and methodology available to journalists, researchers, regulators, and policymakers on request.
About the Author
Ashkon Pour-Heidary, HBSc Neuroscience
Ashkon is the founder of Coast2Coast First Aid and a certified Instructor Trainer for both the American Red Cross and the Canadian Red Cross, as well as an Emergency Medical Responder Instructor Trainer. He holds a Bachelor of Science in Neuroscience from the University of Toronto and has led the certification of more than 150,000 individuals across North America. His work focuses on closing the gap between holding a certificate and being genuinely ready to respond.
Being a lifeguard is about more than just a whistle and a high chair—it’s about being the most prepared person on the pool deck. From mastering lifeguard CPR certification to handling specialized pediatric emergencies, discover why American Red Cross training is the ultimate professional standard.
The California Good Samaritan Act is designed to protect people who provide emergency care or assistance in good faith and without compensation. This article explains what the law covers, who it protects, and what it means for everyday people who want to help in emergencies.
CPR isn’t just for doctors or first responders, it’s a lifesaving skill anyone can learn. This blog explores the importance of CPR training, who should learn it, how CPR saves lives, and why community-wide preparedness matters.
First aid education gives students the confidence and skills to respond in emergencies. Discover why US schools should integrate first aid into their curriculum and how it benefits students, staff, and entire communities.
First aid education gives students the confidence and skills to respond in emergencies. Discover why US schools should integrate first aid into their curriculum and how it benefits students, staff, and entire communities.
Whether you drive professionally or just for daily errands, knowing basic first aid can save lives. From handling car accidents to keeping a well-stocked car first aid kit, this guide shares essential first aid for drivers, practical road safety tips, and why certification with Coast2Coast First Aid & Safety is a smart move for every driver.
Every parent wants to keep their child safe, but accidents can happen in seconds. Learning pediatric first aid and infant CPR gives you the skills and confidence to respond in an emergency. From choking to breathing issues, discover why every parent should be prepared with life-saving knowledge.
Construction is one of the most dangerous industries in the U.S. Discover the top workplace injuries that occur on job sites and why first aid and CPR training are essential for safety and compliance. Learn how Coast2Coast First Aid & Safety’s OSHA-aligned courses can prepare you and your crew to handle emergencies with confidence.